Modelling a Best Practice Approach to Co-Design for Mental Health System Reform
-
2022
-
Service
Public Sector Services
Designed By:
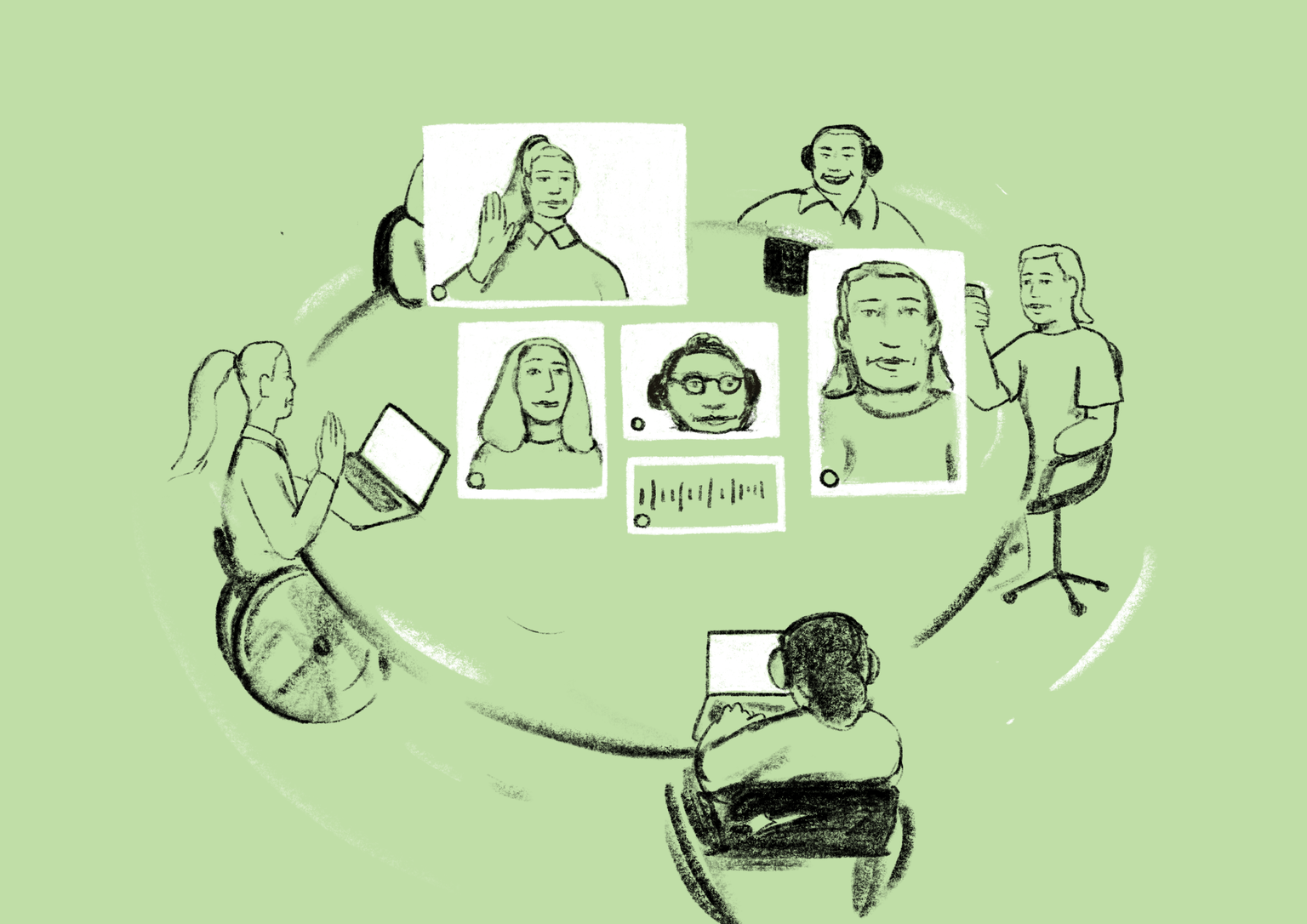
Victoria’s Royal Commission into the State’s mental health system found it was falling “catastrophically short of expectations”, specifically recommending that people with lived experience participate in its transformation. Today partnered with Mental Health Reform Victoria to design safe, practical, scalable ways for people with lived experience to reform the system.